一、前言
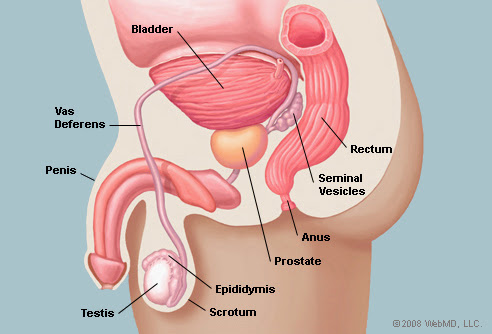
攝護腺,又稱前列腺,在男性膀胱出口,能製造液體以構成精液的一部份。攝護腺癌是全世界男性第二多的癌症,尤其是使用攝護腺特異抗原prostate-specific antigen (PSA)篩檢後。
二、分區
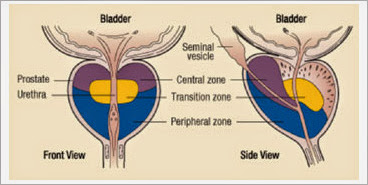
過渡區(Transition zone)/黏膜區(Mucosal gland):包圍近端尿道;分泌量僅占5%;年紀大時,此部位易增生並擠壓尿道,即前列腺肥大,常引發排尿困難
中央區(Central zone)/黏膜下區(Submucosal gland):包圍二個射精管;分泌量約占20~ 25%
周邊部份(Peripheral/ Principal portion):佔分泌量70%,為主要的分泌來源;屬於複合式腺體(compound tubuloalveolar gland)(30~ 50 glands;切面為不規則狀),經由15~ 30個導管(ducts)送至尿道前列腺部
三、臨床症狀
早期通常沒有任何症狀。開始出現症狀時,可能和良性攝護腺肥大(BPH)症狀差不多,包括尿急、開始排尿時排不出來、尿流變細、尿完後滴尿、尿流斷斷續續、膀胱無法排空的感覺、夜尿、血尿等。當攝護腺癌侵犯貯精囊,會出現精液帶血或射精疼痛。若有骨轉移時會引起骨骼疼痛、病理性骨折或脊椎受到壓迫而產生神經方面的症狀。部份患者癌症已擴散至別的器官時才發現。
四、風險因素
1. 年齡: <40歲機率相當低
2. 種族: 非裔美國人最多
3. 基因: 尤其是DNA修復基因(如BRCA2)中的種系突變
其他因素影響較有限
五、診斷
1. 肛門觸診
2. 攝護腺特異抗原prostate-specific antigen (PSA)篩檢
3. 攝護腺超音波
4. 攝護腺切片檢查
5. 骨骼掃瞄、電腦斷層攝影或核磁共振攝影: 主要用來看轉移
六、攝護腺癌分期
六之一: 根據the American Joint Committee on Cancer (AJCC) tumor, node, metastasis (TNM) system
1. Primary tumor (T)
Clinical (cT) 臨床T分期
TX: Primary tumor cannot be assessed
T0: No evidence of primary tumor
T1: Clinically inapparent tumor not palpable or visible by imaging: 在肛門指診摸不到或影像看不到,手術後意外發現或因PSA上升做切片發現
T1a: Tumor incidental histologic finding in ≤5% of tissue resected (at time of transurethral resection of the prostate [TURP])
T1b: Tumor incidental histologic finding in >5% of tissue resected (at time of TURP)
T1c: Tumor identified by needle biopsy (because of elevated prostate specific antigen [PSA] level)
T2: Tumor confined within prostate: 腫瘤侷限在攝護腺分葉中
T2a: Tumor involves one-half of 1 lobe or less
T2b: Tumor involves more than one-half of 1 lobe but not both lobes
T2c: Tumor involves both lobes
T3: Tumor extends through the prostatic capsule: 腫瘤吃出攝護腺的外膜(包含儲精囊)
T3a: Extracapsular extension (unilateral or bilateral)
T3b: Tumor invading seminal vesicle(s)
T4: Tumor fixed or invades adjacent structures other than seminal vesicles (eg, bladder, levator muscles, and/or pelvic wall)腫瘤跑到除了攝護腺及儲精囊外的任何地方
Pathologic (pT) 病理T分期,類似但是病理分期不會有T1
pT2: Organ confined
pT3: Extraprostatic extension
pT3a: Extraprostatic extension or microscopic invasion of the bladder neck
pT3b: Seminal vesicle invasion
pT4: Tumor is fixed or invades adjacent structures other than the seminal vesicles (eg, bladder, rectum)
2. Regional lymph nodes (N)
Clinical (cN) 臨床N分期
NX: Regional lymph nodes were not assessed
N0: No regional lymph node metastasis
N1: Metastasis in regional lymph node(s): 近端淋巴轉移
Pathologic (pN) 病理N分期
pNX: Regional nodes not sampled
pN0: No positive regional nodes
pN1: Metastases in regional nodes(s)
3. Distant metastasis (M)
M0: No distant metastasis
M1: Distant metastasis
M1a: Nonregional lymph nodes(s): 遠端淋巴轉移
M1b: Bone(s): 骨轉移
M1c: Other site(s) with or without bone disease: 其他器官轉移

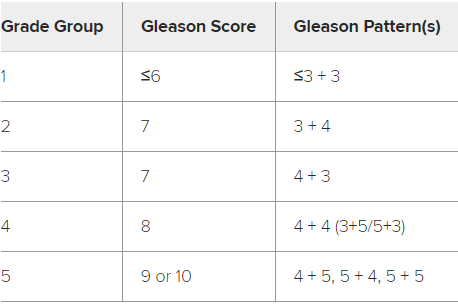
六之二: Gleason Score: 取最大及次大的組織,依分化程度評1-5分,1是正常組織,5是未分化組織,再將兩者相加得出分數
GX: Gleason score cannot be assessed
Gleason ≤6: Well differentiated (slight anaplasia)
Gleason 7: Moderately differentiated (moderate anaplasia)
Gleason 8-10: Poorly differentiated or undifferentiated (marked anaplasia): 8-10基本上認為是預後最差的情況
七、如何選擇治療方式
1. 癌症分期tumor, node, metastasis [TNM] stage
2. 組織分期Gleason score/grade group
3. 血液中PSA濃度
4. 對治療的預期療效及副作用評估
5. 患者的病史、用藥、身體狀況
NCCN提出的風險分層Risk stratification,主要根據下面四項的結果分成6群患者
1. Digital rectal examination (DRE) findings: 肛門指診
2. Prostate-specific antigen (PSA) value: 攝護腺特異抗原指數
3. Biopsy findings: 切片發現
4. Imaging study results: 影像結果

第一組NCCN very low risk: 切片意外發現,組織分化良好,PSA沒上升,切片中腫瘤影響部分<50%
如果患者預期壽命大於10年,則積極監測active surveillance追蹤,部分患者依然可以選擇放射治療或根治性前列腺切除術RT or radical prostatectomy
第二組NCCN low risk: 攝護腺無腫瘤或其中一葉,組織分化良好,PSA沒上升
治療選擇在了解各治療方式的優缺點後以患者選擇決定。
大部分還是以積極且連續性的監測,發現疾病進展再做治療為主,積極監測也可以降低心理壓力。
如果有較高機率疾病進展的患者可以選擇放射治療或根治性前列腺切除術RT or radical prostatectomy(RP),放射治療可以選擇體外放射治療或近接治療external beam source(EBRT) or brachytherapy,EBRT就是傳統的放射治療,近接治療則是植入(1)永久性核種: 碘I-125, Pallium-103等或(2)暫時性核種: 銥Ir-192。根治性前列腺切除術可採用開放式或微創方法進行,區域性淋巴廓清也是選項之一。
目前英國做的大型隨機研究ProtecT中,RT或RP或積極監測對存活率是沒有影響的。
第三組、第四組NCCN intermediate risk: 腫瘤侷限在攝護腺中或Gleason 7分或PSA稍微上升10-20 ng/mL,Favorable跟Unfavorable差在切片中腫瘤是否超過50%
依然分成放射治療跟手術治療,RT可以選擇體外放射治療或近接治療,建議加上雄激素剝奪療法 androgen deprivation therapy(ADT)。手術則是RP加上骨盆腔淋巴結廓清術pelvic lymph node dissection,是否需要術後放射治療則是以病理報告做決定。
在風險相對較低的患者還是可以選擇積極監測。
第五組NCCN high risk: 腫瘤吃到bladder neck或Gleason 8 or 4+5或PSA顯著上升>20 ng/mL
放射治療選擇EBRT+-brachytherapy,並且使用18-36個月的ADT治療。手術則是RP加上骨盆腔淋巴結廓清術pelvic lymph node dissection,淋巴結轉移node-positive的患者可以使用術後RT或ADT。
如果患者預期壽命有限且又局部症狀,單獨使用ADT是可以考慮的。
第六組NCCN very high risk: 腫瘤吃到非攝護腺的器官(包含儲精囊)或Gleason 8-10
侵犯到淋巴結的機率高,須接受CT或MRI骨盆攝影。
放射治療選擇EBRT+-brachytherapy,並且使用18-36個月的ADT治療。在年輕患者可以選擇手術RP加上骨盆腔淋巴結廓清術pelvic lymph node dissection
追蹤可藉由3-6個月一次的PSA及肛門指診。
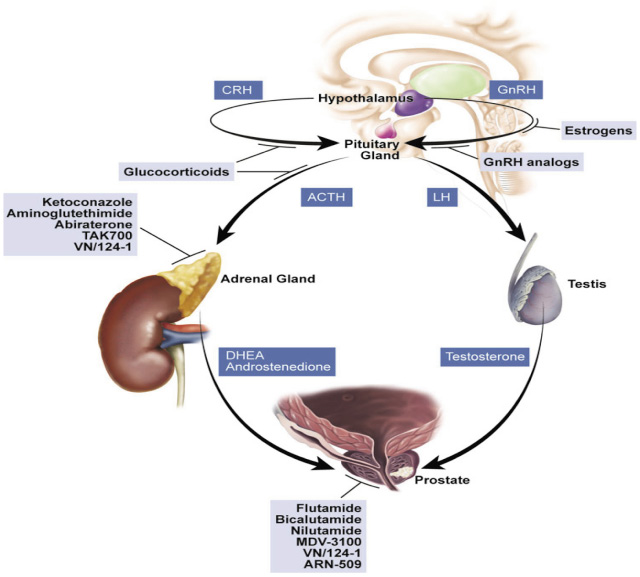
八、雄激素剝奪療法 androgen deprivation therapy(ADT)

1. 促性腺激素釋放荷爾蒙致效劑 (gonadotropin-releasing hormone agonist, GnRH agonist),又稱作促黃體素釋放荷爾蒙致效劑 (luteinizing hormone-releasing hormone agonist, LHRH agonist)
leuprolide 和 goserelin,作用在腦下垂體前葉向下調控 GnRH 受體,降低促黃體素 (luteinizing hormone, LH) 的釋放並減少睪固酮的生成
2. 抗雄激素藥物,又稱做雄激素受體阻斷劑 (androgen receptor antagonist)
依照其結構分為固醇類 (如 cyproterone) 及非固醇類 (如 flutamide, bicalutamide, nilutamide) 兩種,藉由與前列腺細胞上的雄激素受體結合,達到阻斷雄激素的作用。
九、治療副作用
1. ADT: 心血管疾病、葡萄糖代謝受損,身體形象改變和骨質疏鬆症
2. RT: 胃腸道毒性、繼發性惡性腫瘤(機率低)
長期泌尿道問題、性功能障礙
Reference:
1. Uptoate
2. 晚期前列腺癌之合併雄激素阻斷法,藥學雜誌電子報123期
3. 小小整理網站


 留言列表
留言列表
